
Overview
Anxiety disorders are among the most common mental health conditions in Australia. According to the Australian Bureau of Statistics’ National Study of Mental Health and Wellbeing (2020–2022), anxiety disorders affect 17.2 per cent of Australians aged 16 to 85 years in any given 12-month period – equivalent to approximately 3.4 million people. Across a lifetime, 28.8 per cent of Australians – more than one in four – will experience an anxiety disorder at some point.
Anxiety itself is a normal human response to stress and perceived threat. A certain level of anxiety – before a job interview, a medical procedure, or an important decision – is a healthy and functional reaction. Problems arise when anxiety becomes persistent, disproportionate to the situation, and begins to interfere with daily life. At this point, a clinical anxiety disorder may be present.
Anxiety disorders encompass a range of conditions including generalised anxiety disorder (GAD), panic disorder, social anxiety disorder, specific phobias, agoraphobia, and others. They are highly treatable. With appropriate professional support – including psychological therapy, medication where indicated, and self-management strategies – most people with anxiety disorders achieve significant and lasting improvement in their symptoms and quality of life.
Key Terms
- Anxiety disorder : A clinical condition in which anxiety is persistent, disproportionate to the situation, and significantly disrupts daily functioning. Diagnosed using ICD-11 or DSM-5 criteria.
- Amygdala : A small, almond-shaped region in the brain that detects threats and triggers the stress response. In anxiety disorders, the amygdala may become hyperactivated.
- Fight-or-flight : The body’s automatic survival response to perceived danger. Controlled by the hypothalamus and adrenal glands, it raises heart rate, increases breathing, and releases adrenaline.
- GAD : Generalised Anxiety Disorder – excessive, uncontrollable worry about a range of everyday topics, present on most days for at least 6 months.
- Comorbidity : The presence of two or more health conditions at the same time. Anxiety disorders frequently co-occur with depression, PTSD, OCD, and chronic pain.
Symptoms
Symptoms of anxiety disorders vary depending on the type of disorder and the individual. Not everyone will experience the same combination of symptoms. In general, anxiety disorders produce a characteristic mix of physical, emotional, cognitive, and behavioural symptoms.
Physical Symptoms
Physical symptoms are common in anxiety disorders and can sometimes be confused with medical conditions. They include:
- Rapid or irregular heartbeat.
- Chest tightness or chest discomfort.
- Shortness of breath.
- Sweating or trembling.
- Dizziness or lightheadedness.
- Stomach pain, nausea, or loose bowel movements.
- Muscle tension, particularly in the shoulders and neck.
- Headaches.
- Fatigue.
- Difficulty sleeping or frequent waking.
Emotional Symptoms
- Persistent worry or fear, often without a clear cause.
- Irritability or feeling constantly on edge.
- Feeling overwhelmed by everyday tasks.
- A sense that something bad is about to happen.
- Difficulty relaxing.
- Reduced enjoyment of activities previously enjoyed.
Cognitive Symptoms
- Difficulty concentrating or staying on task.
- Repetitive negative thoughts.
- Catastrophic thinking – expecting the worst outcome in most situations.
- Overestimating the likelihood or severity of threats.
- Difficulty making decisions.
Behavioural Symptoms
- Avoiding people, places, or situations that trigger anxiety.
- Withdrawing from social activities.
- Repeatedly seeking reassurance from others.
- Difficulty starting or completing tasks.
- Increased use of alcohol or other substances to manage feelings.
When to See a Doctor
See your GP if anxiety symptoms are persistent, significantly affecting your daily life, relationships, work, or study, or do not improve with self-management strategies over several weeks.
Seek urgent help if you are experiencing panic attacks, are unable to leave your home due to anxiety, or are having thoughts of self-harm. Contact Lifeline on 13 11 14 (24/7) or the Suicide Call Back Service on 1300 659 467.
In Australia, a GP can assess your symptoms, refer you for psychological therapy under a GP Mental Health Treatment Plan (up to 10 Medicare-rebated sessions per year with a psychologist), and discuss whether medication may be appropriate for your situation. You may also contact Truewell Clinic directly at truewellclinic.com.au for a confidential psychiatric assessment and anxiety treatment.
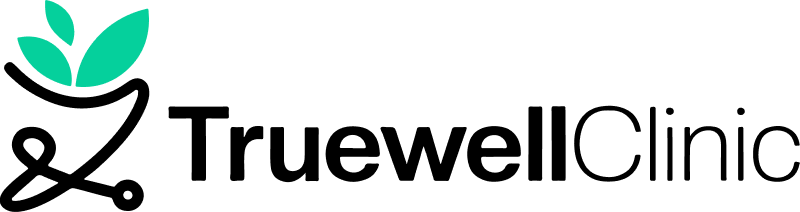
Types of Anxiety Disorders
The term ‘anxiety disorder’ covers several distinct conditions. A GP or mental health professional can identify the specific type affecting a person, which guides the most effective treatment approach.
Generalised Anxiety Disorder (GAD)
Excessive, difficult-to-control worry about a wide range of everyday matters – health, finances, relationships, work, or daily responsibilities. Worry is present on most days for at least 6 months. Affecting approximately 3 per cent of Australians, GAD is one of the most common anxiety disorders in the country.
Panic Disorder
Recurrent, unexpected panic attacks – sudden surges of intense fear with prominent physical symptoms including racing heartbeat, shortness of breath, chest pain, dizziness, and a sense of losing control or dying. People with panic disorder often develop significant anxiety about having further attacks.
Social Anxiety Disorder (Social Phobia)
Intense fear of social situations due to concern about being judged, embarrassed, or humiliated. Can affect everyday activities including speaking at work, eating in public, or meeting new people. Social phobia has increased in prevalence from 4.7 per cent to 7.3 per cent of Australians between 2007 and 2023 (AIHW).
Agoraphobia
Fear of being in situations where escape might be difficult or help unavailable during a panic attack – such as crowds, public transport, open spaces, or being outside the home alone. Agoraphobia has increased from 2.8 per cent to 4.5 per cent prevalence in Australia (AIHW Burden of Disease 2024).
Specific Phobia
An intense, irrational fear of a specific object, animal, or situation – such as heights, spiders, injections, or flying – that is disproportionate to any actual danger and leads to avoidance behaviour.
Separation Anxiety Disorder
Excessive fear or distress about separation from attachment figures – most commonly seen in children but also occurring in adults. Separation from a caregiver or loved one triggers significant anxiety beyond what is developmentally appropriate.
Health Anxiety (Illness Anxiety Disorder)
Preoccupation with having or developing a serious illness, in the absence of medical evidence. Previously referred to as hypochondria. Characterised by frequent self-examination, repeated medical consultations, and difficulty being reassured by normal test results.
Obsessive-Compulsive Disorder (OCD)
Recurring, intrusive thoughts (obsessions) that cause significant distress, combined with repetitive behaviours or mental acts (compulsions) performed to temporarily reduce that distress. OCD creates a self-reinforcing cycle that can significantly disrupt daily life.
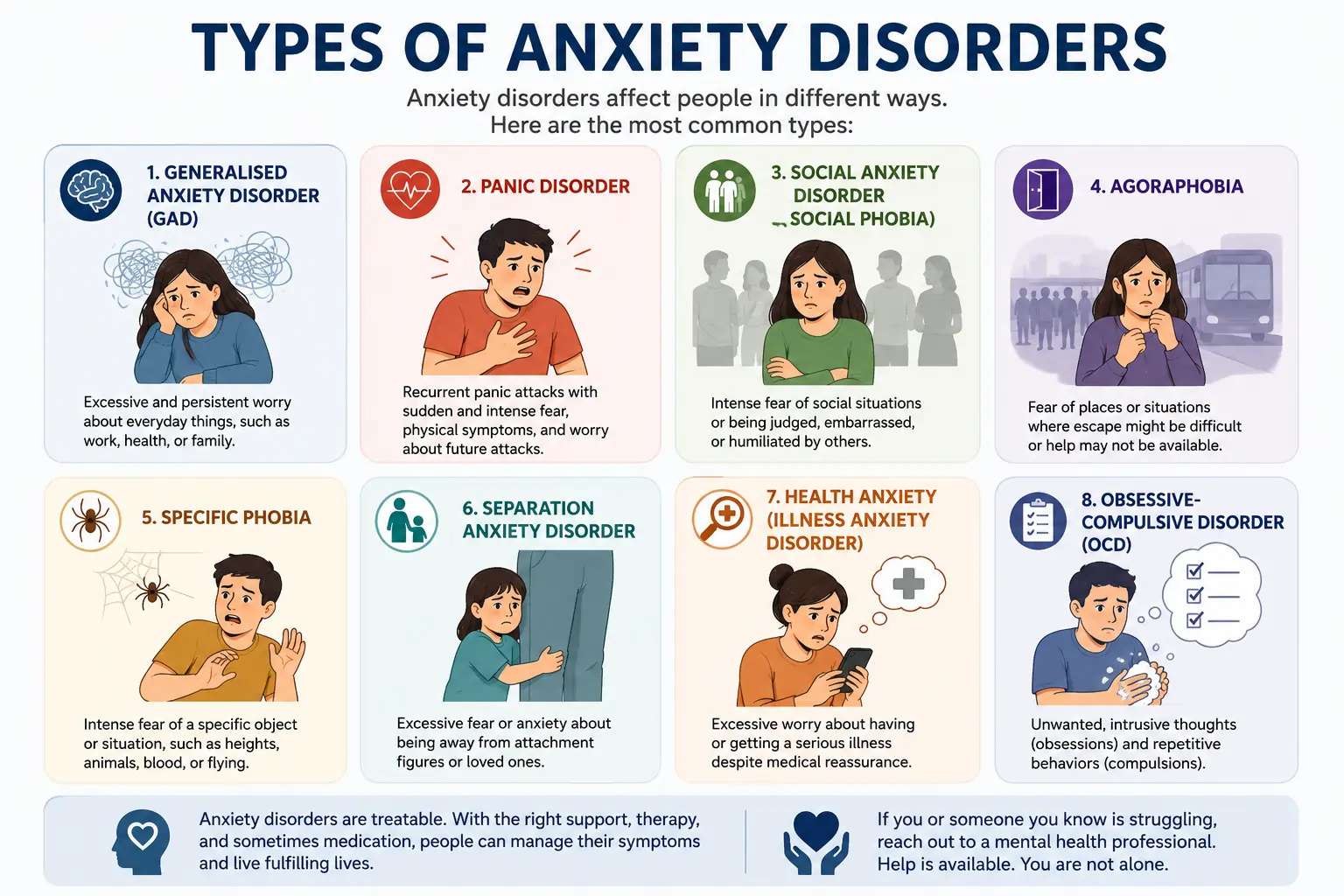
Causes
Anxiety disorders do not arise from a single cause. Research consistently indicates that they develop from a combination of genetic vulnerability, environmental experiences, physiological factors, and life circumstances. Understanding causes helps to reduce stigma and identify appropriate pathways to support.
- Genetic factors. Anxiety disorders can run in families. A first-degree relative with an anxiety disorder increases a person’s risk. Genetics influence how the brain regulates the stress response, neurotransmitter activity, and emotional reactivity – making some individuals more biologically predisposed to anxiety.
- Brain chemistry and structure. Anxiety disorders are associated with dysregulation of neurotransmitters – chemical messengers in the brain including serotonin, noradrenaline, and gamma-aminobutyric acid (GABA). The amygdala, which processes threat and fear, may be hyperactivated in people with anxiety disorders, triggering the fight-or-flight response more readily.
- Stressful or traumatic life events. Exposure to trauma, abuse, neglect, loss, or prolonged stress can trigger or significantly worsen anxiety disorders. Childhood adversity in particular is associated with long-term changes in how the nervous system responds to perceived threats.
- Medical conditions. Certain medical conditions produce symptoms that overlap with anxiety or can directly cause anxiety, including thyroid disorders, heart arrhythmias, respiratory conditions, and chronic pain. A full medical evaluation is important when anxiety is first assessed.
- Substance use and withdrawal. Alcohol, cannabis, stimulants, and other substances can cause anxiety symptoms or worsen existing anxiety disorders. Anxiety is also a well-recognised withdrawal symptom from alcohol, benzodiazepines, and antidepressants if discontinued abruptly.
- Co-occurring mental health conditions. Anxiety frequently co-occurs with depression, PTSD, OCD, ADHD, and other mental health conditions. Addressing all co-occurring conditions is important for effective treatment.
Risk Factors
Certain factors may increase the likelihood of developing an anxiety disorder. These include:
- Female sex. Females are approximately 1.6 times more likely than males to experience a 12-month anxiety disorder in Australia. ABS data (2020–2022) shows a 12-month prevalence of 21.1 per cent in females compared with 13.3 per cent in males.
- Younger age. Australians aged 16–24 have the highest rates of any mental disorder, with 38.8 per cent reporting a 12-month mental disorder in 2020–2022. Anxiety is the most commonly reported condition in this group.
- Childhood trauma or adverse experiences. Children who experience abuse, neglect, or traumatic events are significantly more likely to develop anxiety disorders in later life.
- Family history. A family history of anxiety disorders, depression, or other mental health conditions is a risk factor.
- Personality traits. Traits including high neuroticism, perfectionism, and a tendency toward negative thinking are associated with increased vulnerability to anxiety.
- Chronic physical health conditions. Living with a serious or chronic physical health condition – particularly conditions involving pain, uncertainty, or significant lifestyle impact – is associated with higher rates of anxiety.
- Substance use. Use of, or withdrawal from, alcohol, cannabis, or stimulants increases anxiety risk.
- Academic and occupational pressure. Australian data show elevated anxiety rates in students and workers in high-demand environments. Approximately 35.9 per cent of Australian secondary school students reported high levels of anxiety or depression in 2023 (Resilient Youth Australia).
Anxiety Across Different Groups in Australia
Children and Adolescents
Anxiety disorders are the most common mental health condition in Australian children and adolescents. ABS data estimates that approximately 6.9 per cent of children aged 4–17 experience an anxiety disorder. Among secondary school students, 35.9 per cent reported high levels of anxiety or depression in the 2023 Resilient Youth Australia State of the Nation Report – a rate that has not improved since the COVID-19 disruption years of 2021 and 2022.
Separation anxiety and specific phobias are more common in younger children. Generalised anxiety disorder and social anxiety disorder become more prevalent in adolescence, particularly from around 12 to 14 years of age. Girls show higher rates of anxiety than boys from adolescence onwards, consistent with adult patterns.
Australian Youth Support Services
Headspace (headspace.org.au) provides free or low-cost mental health support for young Australians aged 12–25, with over 160 centres nationally and digital services available Australia-wide. Kids Helpline (1800 55 1800) provides free 24/7 counselling for people aged 5–25.
Students
Anxiety is widespread among Australian university and TAFE students. Performance anxiety, academic pressure, financial stress, and social challenges all contribute. ABS data show that 16 per cent of female students and approximately 8 per cent of male students report signs consistent with generalised anxiety disorder. Social anxiety disorder affects approximately 10 per cent of female students and 4.9 per cent of male students at university level.
Most Australian universities and TAFE institutions offer free counselling services. Students can also access mental health support through university health centres, the Beyond Blue Student Wellbeing portal, and Headspace.
Workplace Anxiety in Australia
Workplace-related anxiety is a significant issue in Australia. Safe Work Australia data indicates that approximately 12 per cent of Australian workers report that anxiety or psychological distress affects their work capacity. Mental health conditions – including anxiety – are the second most common cause of long-term work absence in Australia. Compensation claims related to mental health conditions have increased year on year.
Employers have a legal obligation under Australian work health and safety legislation to address psychosocial hazards – workplace factors that contribute to anxiety, stress, and other mental health conditions. The Black Dog Institute and Beyond Blue both provide workplace mental health resources for Australian employers and employees.
Anxiety During Pregnancy and the Perinatal Period
Approximately 15–20 per cent of Australian women experience anxiety during pregnancy or in the postnatal period. This is higher than the general population rate and often co-occurs with perinatal depression. PANDA (Perinatal Anxiety and Depression Australia – panda.org.au) provides free, specialist telephone support for families affected by perinatal anxiety and depression.
Older Australians
Anxiety in older Australians is often underdiagnosed. ABS data show a prevalence of anxiety symptoms in 16–18 per cent of women aged 60–79 and 8–11 per cent of men in the same age group. Anxiety in older adults is frequently associated with chronic health conditions, bereavement, social isolation, and concerns about independence.
Diagnosis
A GP is the recommended first point of contact for anyone in Australia who is concerned about anxiety symptoms. A comprehensive assessment is important to ensure an accurate diagnosis and to rule out medical conditions that may produce similar symptoms.
Diagnosis of anxiety disorders in Australia uses criteria from the International Classification of Diseases (ICD-11), published by the World Health Organisation, or the Diagnostic and Statistical Manual (DSM-5). Both systems require that symptoms are persistent, clinically significant, and cause meaningful impairment to daily functioning.
Assessment Process
- Clinical interview. A GP or mental health professional takes a detailed history of symptoms, their duration, severity, and impact on daily life.
- Validated screening tools. Standardised questionnaires such as the Generalised Anxiety Disorder 7-item scale (GAD-7) and the Patient Health Questionnaire for Anxiety and Depression (PHQ-4) are commonly used in Australian primary care.
- Medical investigations. Blood tests and other investigations may be ordered to exclude medical causes of anxiety symptoms, including thyroid disorders, anaemia, and cardiac arrhythmias.
- Differential diagnosis. A qualified clinician rules out other mental health conditions that may produce similar symptoms, and identifies any co-occurring conditions such as depression, PTSD, or OCD.
- Specialist referral. Where indicated, a GP may refer to a psychiatrist or psychologist for more detailed assessment, particularly for complex presentations or treatment-resistant anxiety.
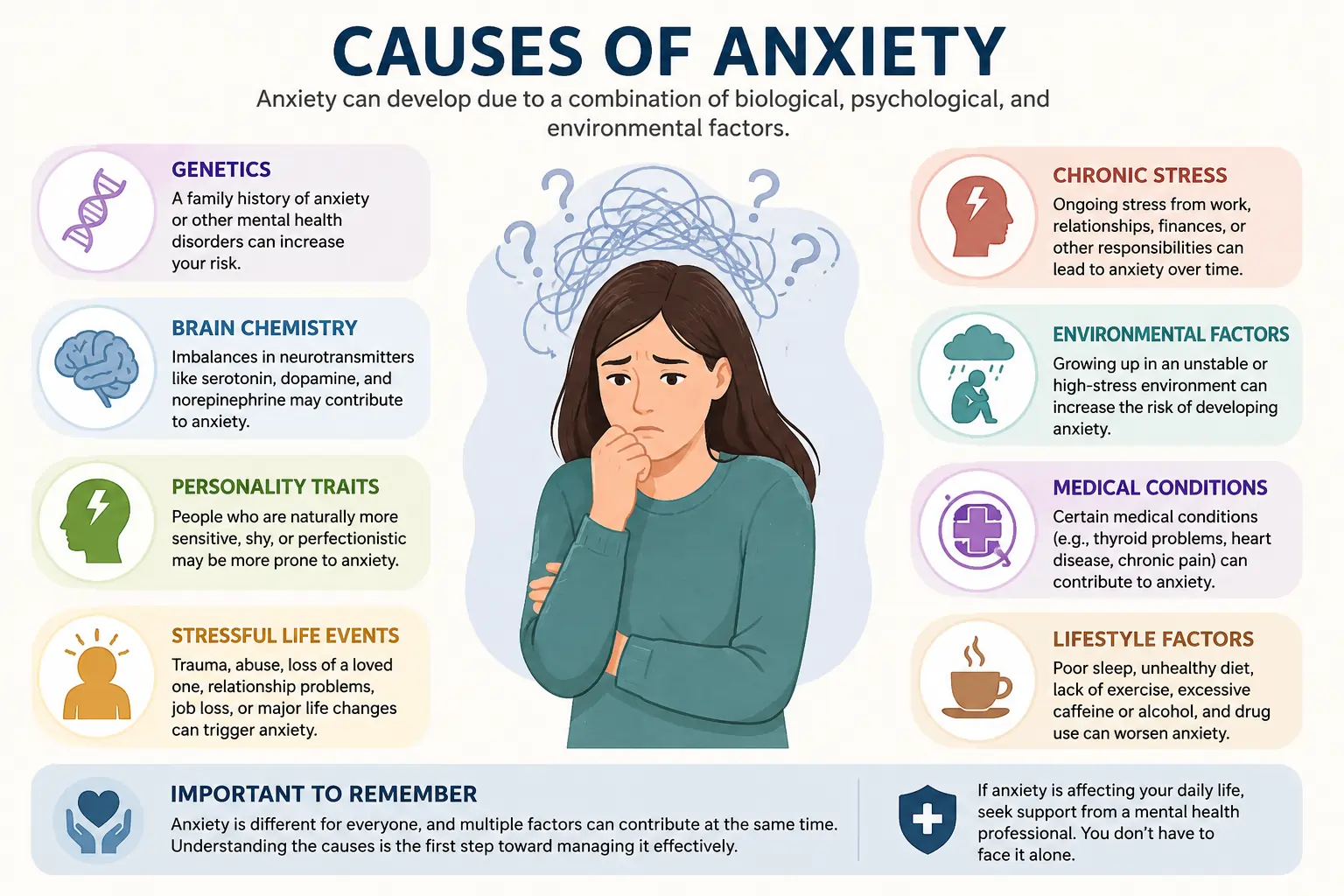
Treatment
Anxiety disorders are among the most treatable mental health conditions. The evidence base for anxiety treatment is strong and consistently demonstrates that most people achieve meaningful improvement with appropriate care. Treatment is typically individualised and may combine psychological therapy, medication, and self-management strategies.
Psychological Therapies
- Cognitive Behavioural Therapy (CBT). CBT is the most extensively researched and evidence-supported psychological treatment for anxiety disorders. It works by identifying and challenging unhelpful thought patterns and gradually modifying anxiety-maintaining behaviours. CBT for anxiety in Australia is typically delivered over 8–12 sessions with a registered psychologist or accredited CBT therapist.
- Exposure Therapy. A component of CBT for many anxiety disorders, exposure therapy involves gradual, systematic, and safe exposure to feared situations or stimuli. It reduces avoidance and desensitises the anxiety response over time. It is particularly effective for specific phobias, social anxiety disorder, OCD, and PTSD.
- Acceptance and Commitment Therapy (ACT). ACT helps people change their relationship with anxious thoughts rather than trying to eliminate them. It builds psychological flexibility and values-based action. ACT has strong evidence for anxiety disorders and is increasingly used by Australian psychologists.
- Mindfulness-Based Cognitive Therapy (MBCT). Combines mindfulness practices with CBT principles. Particularly useful for preventing relapse in people with recurrent anxiety and depression.
Medications
Medication is not required for all people with anxiety disorders, but can be an effective component of treatment for moderate to severe conditions, or when psychological therapy alone is insufficient. Medication is prescribed and monitored by a GP or psychiatrist.
- Selective serotonin reuptake inhibitors (SSRIs). First-line medication treatment for most anxiety disorders in Australia. Examples include sertraline, escitalopram, and fluoxetine. SSRIs are taken daily and typically take 4–6 weeks to show full effect.
- Serotonin-noradrenaline reuptake inhibitors (SNRIs). A second class of antidepressant medicines also used for anxiety disorders, including venlafaxine and duloxetine.
- Benzodiazepines. Sometimes prescribed for short-term relief of severe anxiety symptoms. Not recommended for long-term use due to risks of dependence and tolerance.
- Buspirone. A non-benzodiazepine anti-anxiety medicine used for GAD. Does not carry the dependence risk of benzodiazepines.
Self-Management Strategies
Self-management strategies are a valuable complement to professional treatment and are supported by evidence for improving anxiety symptoms. They include:
- Regular physical activity. A minimum of 150 minutes of moderate-intensity exercise per week is recommended. Exercise reduces anxiety through its effects on stress hormones, neurotransmitters, and the hypothalamic-pituitary-adrenal axis. Even 30 minutes of brisk walking most days shows measurable benefits.
- Sleep regulation. Anxiety and sleep are closely linked. Consistent sleep and wake times, limiting screen exposure before bed, and avoiding caffeine after midday support healthy sleep and reduce cortisol elevation associated with sleep disruption.
- Diaphragmatic breathing exercises. Slow, controlled breathing activates the parasympathetic nervous system – the body’s calming response – and reduces the physical symptoms of anxiety. Various breathing techniques are available through the Beyond Blue, Head to Health, and Headspace platforms.
- Progressive muscle relaxation (PMR). PMR involves systematically tensing and releasing muscle groups to reduce physical tension and interrupt the anxiety response. Guided PMR audio resources are freely available online.
- Structured routine and planning. Organising daily tasks with a planner or digital calendar, breaking tasks into smaller steps, and setting realistic deadlines reduces the sense of overwhelm that can escalate anxiety.
- Limiting alcohol and caffeine. Both substances can worsen anxiety – alcohol through rebound anxiety during withdrawal, and caffeine through its direct stimulant effects on the nervous system.
- Social connection. Maintaining regular contact with trusted friends, family, or community groups provides emotional regulation support and reduces social isolation, a significant risk factor for worsening anxiety.
Complications of Untreated Anxiety
Without appropriate treatment, anxiety disorders can worsen over time and contribute to a range of additional mental and physical health complications. These may include:
- Depression – the most common co-occurring condition with anxiety disorders.
- Substance use disorders – alcohol or drug use as attempts to manage anxiety symptoms.
- Sleep disorders, including chronic insomnia.
- Digestive conditions, including irritable bowel syndrome (IBS).
- Cardiovascular effects – chronic stress and anxiety are associated with elevated blood pressure and increased cardiovascular risk.
- Reduced academic and occupational functioning.
- Social isolation and relationship difficulties.
- Reduced quality of life.
- In severe cases, suicidal ideation.
Prevention
Anxiety disorders cannot always be prevented. However, several strategies can reduce risk and improve resilience:
- Seek early support after traumatic or stressful life events – early intervention reduces the likelihood of anxiety disorders developing or becoming chronic.
- Maintain regular physical activity, adequate sleep, and a balanced diet.
- Develop stress management skills – including mindfulness, relaxation techniques, and problem-solving.
- Limit alcohol and substance use.
- Build and maintain social connections.
- Speak with a GP or pharmacist before starting any new medicine or supplement, as some can worsen anxiety symptoms.
- Access workplace or school support programs early when anxiety begins to affect performance.
References
- Australian Bureau of Statistics. National Study of Mental Health and Wellbeing 2020–2022. ABS. abs.gov.au. Released October 2023. Accessed June 2026.
- Australian Institute of Health and Welfare. Mental Health Overview. AIHW. aihw.gov.au/mental-health/overview. Updated 2024. Accessed June 2026.
- Australian Institute of Health and Welfare. Australian Burden of Disease Study 2023. AIHW. aihw.gov.au. Published 2024. Accessed June 2026.
- Beyond Blue. Australia’s Mental Health and Wellbeing Check 2024. beyondblue.org.au. Accessed June 2026.
- Resilient Youth Australia. State of the Nation Report 2023: Wellbeing of Australian Young People. resilienceeducation.com.au. 2023.
- Walsh L, et al. The 2024 Australian Youth Barometer: Understanding Young People in Australia Today. Monash University, Centre for Youth Policy and Education Practice. 2024.
- Safe Work Australia. Psychological Health in Australian Workplaces: Work-Related Psychological Health and Safety. safeworkaustralia.gov.au. 2022.
- National Mental Health Commission. National Report Card on Mental Health and Suicide Prevention 2023. mentalhealthcommission.gov.au. 2023.
- Healthdirect Australia. Anxiety. healthdirect.gov.au/anxiety. Accessed June 2026.
- World Health Organisation. ICD-11 – International Classification of Diseases, 11th Revision. who.int/classifications/icd. 2022.
Professional Support at Truewell Clinic
If you are experiencing persistent anxiety that is affecting your daily life, Truewell Clinic (truewellclinic.com.au) offers confidential, evidence-based assessment and treatment of anxiety disorders by experienced psychiatrists. Care is personalised and focused on long-term recovery and improved quality of life.
Services include clinical assessment, CBT and exposure therapy, psychiatric medication review, and ongoing mental health management. Appointments can be booked online at truewellclinic.com.au.
Key Statistics – At a Glance (2026)
12-month anxiety prevalence
Australians affected yearly
Lifetime prevalence
LGBTQI+ 12-month anxiety
MH expenditure (2023–24)
Young adults (18–34)
Six-Year Comparison — Australian Anxiety Statistics (2021–2026)
| Indicator | 2021 | 2022 | 2023 | 2024 | 2025 | 2026 |
|---|---|---|---|---|---|---|
| 12-month anxiety prevalence (% adults 16–85) | ~16.5% (estimate) | 17.2% (data collection period) | 17.2% ✅ ABS Oct 2023 | ~17.5% (est.) | ~18–19% (est.) | Pending ABS GSS mid-2026 |
| Lifetime anxiety prevalence | ~26% | ~27% | 28.8% ✅ | 28.8%+ | 28.8%+ | Pending |
| Females — 12-month anxiety | ~19% | ~20% | 21.1% ✅ | 21.1%+ | Increasing | — |
| Males — 12-month anxiety | ~12% | ~12.5% | 13.3% ✅ | 13.3%+ | Increasing | — |
| LGBTQI+ 12-month anxiety | ~45% | ~48% | 50.3% ✅ | 50%+ | — | — |
| Secondary school students anxiety | ~33% | ~34% | 35.9% ✅ | No improvement | — | — |
| Mental health expenditure (AUD billions) | ~$10.8B | ~$12B | $13.2B | $13.8B ✅ | $14B+ est. | — |
| PBS mental health prescriptions | ~$741M | ~$750M | ~$760M | ~$770M | $781M ✅ | — |
Notes on Data Interpretation
- ⚠️ ABS General Social Survey (GSS) 2025–26 introduces a new baseline. Updated national prevalence data expected mid-2026.
- The 17.2% figure remains the most authoritative confirmed 12-month prevalence statistic for 2026 content use.
- The $13.8B expenditure figure is from the Productivity Commission (Report on Government Services 2026).
- AIHW Burden of Disease updates (2024) reflect long-term trend comparisons, not annual changes.
Verified Source Links
ABS — NSMHW 2020–2022: https://www.abs.gov.au/statistics/health/mental-health/national-study-mental-health-and-wellbeing/latest-release
AIHW Mental Health Overview: https://www.aihw.gov.au/mental-health/overview
AIHW Expenditure: https://www.aihw.gov.au/mental-health/topic-areas/expenditure
Productivity Commission 2026: https://www.pc.gov.au/ongoing/report-on-government-services/health/services-for-mental-health
Monash Youth Barometer 2024: https://www.monash.edu/education/cypep/research/the-2024-australian-youth-barometer
Safe Work Australia: https://www.safeworkaustralia.gov.au/safety-topic/industry-and-business/mental-health-workplace
This article is intended for general informational purposes and does not constitute medical advice. It has been prepared for an Australian audience in accordance with Australian health information standards and the EEAT (Experience, Expertise, Authoritativeness, Trustworthiness) framework. Always consult a registered healthcare practitioner for advice specific to your situation. In a mental health crisis, call Lifeline on 13 11 14 (24 hours, 7 days).


